Definition:
Table of Contents
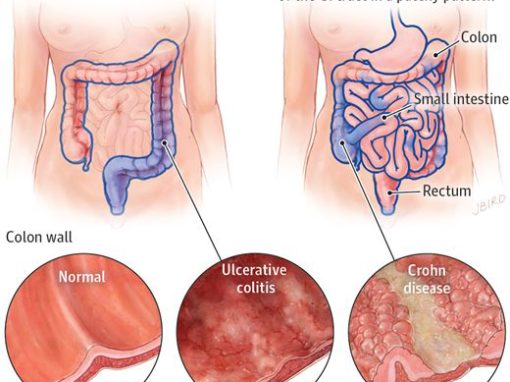
- Chronic inflammation of the bowel that could be due to abnormal immune system response to the enteric flora. There are generally 2 types: Chron’s disease (CD) and Ulcerative colitis (UC).
- Diagnosis of exclusion, bimodal onset (15-25 and 50-80). Chron’s disease usually in 20s and UC in the 40s
- Sub-classified as Ulcerative colitis or Crohn’s disease.
Etiology and Association:
- Abnormal immune response to the flora
- Associated with genetics (HLAB27), infection, abnormal host reactivity
- Associated with dysregulated cytokines (IL-12/IL-23)
Clinical Presentations:
- Common to both IBD: Fever, abdominal pain, tenderness, diarrhea, weight loss, bloody stool).
- Recurrent bouts of bloody mucoid diarrhea (especially Ulcerative colitis), Chrons more watery.
- Lower abdominal pain/cramps – location depends on site affected; Tenesmus (painful defecate)
- Fever, weight loss if severe; anemia of chronic disease
- Symptoms of malabsorption – depending if you talking about UC or CD (CD with steatorrhea due to ↓ bilesalt)
- If small intestine Chrons: features of subacute intestinal obstruction, mass
- Extra-intestinal manifestations (seen in both but more common in Chron’s Disease > UC)
- Joint: Sacrolieitis, Migratory Polyarthritis, Ankylosing Spondylitis,
- Skin: Pyoderma gangrenosum / Erythema nodosum (indicator of disease severity),
- 1o Sclerosing cholangitis, Eyes: Anterior Uveitis iritis
Diagnostic test
- Most accurate test – Endoscopy when can be reach by the scope (UC and Chron’s)
- Barium studies also diagnostic – in both UC and Chron’s.
- If still unclear can use serologic testing
- Chrons disease: ANCA–ve ASCA+ve
- Ulcerative colitis: ANCA+ve ASCA–ve
- CD – mainly in small bowel (never rectum) but most common affect terminal ileum
- UC – always rectum and proximal but never pass the colon.
Complications
- Colorectal Cancer, Toxic megacolon, Cholangiocarcinoma, 1osclerosing cholangitis
- All above both can cause but UC more prone.
- Note that both chrons involving colon and UC can cause colon cancer.
- More common in Chrons: Mass, Upper GIT, Perianal disease (Perianal Abscess and Fistula), hypocalcemia from fat malabsorption, obstruction, kidney stones (CaOx), gall stones (cholesterol), B12 malabsorption.
- Post diagnosis of IBD for 8-10 years you need to screen with colonoscopy every 1-2 years.
Treatment and Management
- Treatment for UC and Chrons depends on the severity of the disease. The severity can be objectively evaluated with the following:
- Chrons disease: severity is objectively measure via CDAI interpretation.
- Asymptomatic remission
- Mild to Moderate active
- Moderate to severely active
- Severely active to fulminant disease.
- Initial Therapy for UC and Chrons
- Mesalamine (not Sulfasalazine) due to side effect: rash, Interstitial nephritis, hemolytic anemia.
- Acute Exacerbation
- Steroids (Prednisone/Budesonide) for both Chrons and UC
- Azathioprine or 6MP to wean patient off steroid [both can cause pancreatitis] in severe cases dependent on steroid. All need vitamin D and Calcium.
- Severe disease:
- Recurrent symptoms when steroids are stopped start
- Azathioprine, 6-mercaptopurine (6-MP), wean off steroid.
- Chronic Maintenance of remission (5-ASA derivatives = mesalamine) different types used
- Mesalamine
- Asacol – UC ; Rowasa – UC (limited to rectum); Pentasa – CD
- Sulfasalazine (obsolete version of mesalamine) can cause Rash, AIN,hemolysis, infertility in men (reversible) and Leukopenia.
- Metronidazole + Ciprofloxacin (perianal disease in chrons)
- Infliximab (Fistula of Chrons or Refractory severe disease of IBD) fistula = severe.
- Need PPD/Quantiferon screen and has Joint pain side effect: TNF cause granuloma, hence inhibit can release TB from granuloma
- If PPD positive (Isoniazid for 9 months) and CXR negative
- No need to wait 9 months to begin therapy infliximab
- Newer drugs active only in colon (Balsalazide, Olsalazine)
- Vedolizumab: IV for moderate to severe IBD not controlled with other medications. Need for induction and maintenance therapy. Better than Natalizumab due to no documented PML.
- Surgery – Curative for UC if refractory to medication. Chrons usually recur at anastomosis but still do due to obstruction/stricture.
- Mesalamine